Great News
Beijing Chunlizhengda Medical Instruments Co., Ltd.'s "Self - Stabilizing Interbody Fusion Cage" has been approved for registration by the National Medical Products Administration (NMPA) of the People's Republic of China
Introduction
The Anterior Lumbar Interbody Fusion (ALIF) technique was first reported in the 1960s. In its early stage, ALIF was mainly used for the treatment of spinal tuberculosis, and later gradually expanded to other related spinal diseases. Despite the continuous evolution of ALIF - related standard technologies and implantable devices with subsequent technological advancements, its core therapeutic principle remains unchanged: resecting the intervertebral disc via an anterior approach, placing a fusion cage or a large bone graft in the intervertebral space to maintain the disc height and anterior vertebral stability, and ultimately achieving bony fusion of the vertebrae.
Definition: Anterior Lumbar Interbody Fusion (ALIF) is a minimally invasive surgical procedure for treating lumbar degenerative diseases. During ALIF, the lumbar spine is accessed from the anterior (front) approach. Most of the degenerated intervertebral disc is removed to relieve compression on the spinal nerves and enlarge the neural foramen. The procedure is termed "anterior" because the spine is exposed from the front.Unlike posterior lumbar surgery (which is performed through the back), anterior surgery avoids damaging the lumbar muscles and preserves the stability of the posterior lumbar structures. After removing the disc, the resulting space is filled with bone graft material to fuse the adjacent vertebrae together, thereby providing supportive function.
Surgical Principles:Typically, an incision is made in the lower abdomen, slightly off the midline toward the left side. For the L5-S1 intervertebral space, a left or right lower abdominal incision may be adopted, and interbody fusion is performed via an oblique approach to expose the anterior aspect of the lumbar spine. Surgical instruments are then used to remove part or all of the degenerated intervertebral disc, enabling neural decompression.
Intervertebral fusion:After removing most of the intervertebral disc, the resulting intervertebral space is filled with a bone graft-containing interbody fusion cage, which replaces the disc. This implant provides stability for new bone ingrowth and fuses the adjacent vertebrae together.
Postoperative care:The incision is then closed and dressed, marking the completion of the surgery. Patients typically remain hospitalized for 2 to 4 days. Strenuous activities should be avoided within 6 to 12 weeks postoperatively.
Surgical procedure
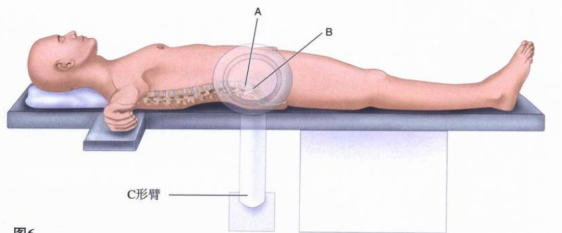
1、Positioning and incision design
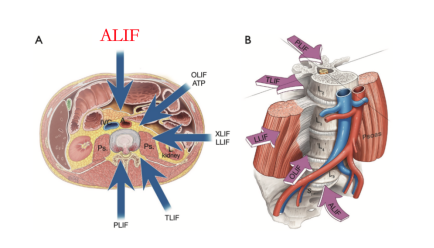
Traditional and Modified Approaches of ALIF.The traditional approaches for Anterior Lumbar Interbody Fusion (ALIF) include the midline transperitoneal approach and the anterolateral retroperitoneal approach. With the advancement of minimally invasive concepts, the traditional approaches have been modified into the mini-open anterior approach. A transverse incision (3-5 cm in length) is made slightly left of the abdominal midline at the corresponding vertebral level, which can be performed via either a transperitoneal or retroperitoneal route.
①The transperitoneal approach, a relatively older technique, is increasingly less commonly used. It carries the risk of injuring the peritoneum and the superior/inferior hypogastric plexuses, as well as may lead to iatrogenic secondary intestinal atrophy surrounding fibrotic scar tissue. However, it remains a viable option for patients in whom retroperitoneal dissection is not feasible due to a history of multiple prior abdominal surgeries, or for those requiring revision surgery via an anterior spinal approach.
② The retroperitoneal approach can be performed via the left or right side at the L5/S1 level. On one hand, it avoids the obstruction of the liver in the surgical field; on the other hand, since the inferior vena cava is located anterior to the right side of the spinal column, the risk of injury to the inferior vena cava during the operation can be reduced.
③ The aponeurosis of the external oblique abdominis is incised, and the fibers of the external oblique abdominis are separated to expose the internal oblique abdominis, transversus abdominis, transversalis fascia, and peritoneum. Extraperitoneal fat is seen bulging from the incision, and the lateral peritoneum, together with the ureter, is retracted toward the midline using saline-soaked gauze until reaching the anterior aspect of the vertebral body. The operation is performed in the triangular area between the bifurcation of the iliac veins and the sacral promontory. If necessary, the median sacral artery is ligated to achieve adequate exposure.
2、Exposed diseased intervertebral disc
Dissect along the intermuscular space from the incision to the peritoneum. Due to the effect of gravity, the peritoneum and blood vessels will shift to one side, indirectly exposing the intervertebral disc. Finally, surgical instruments are used to establish a direct channel to the disc.
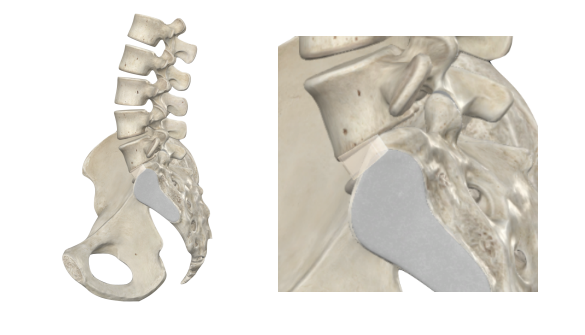
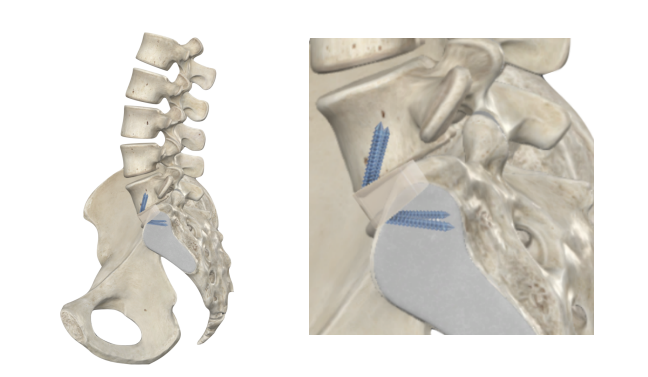
3、Implant intervertebral fusion device
Confirm the surgical level, then completely resect the intervertebral disc. Insert a trial implant of appropriate size, and use C-arm fluoroscopy to verify the suitability of the trial implant's size and angle. Subsequently, place an interbody fusion cage matching the trial implant's size to complete the fusion procedure. The interbody fusion cage for the L5/S1 level is pre-equipped with screws, allowing the entire surgery to be performed through a single incision. This eliminates the need for repositioning the patient to place posterior pedicle screws separately. Artificial bone graft and autologous blood are placed inside the interbody fusion cage to promote intervertebral fusion.
4、Postoperative rehabilitation
Postoperative patients should wear a lumbar brace to limit movement of the lumbar spine, promote fusion, and prevent the intervertebral fusion device from dislodging.
Product Features

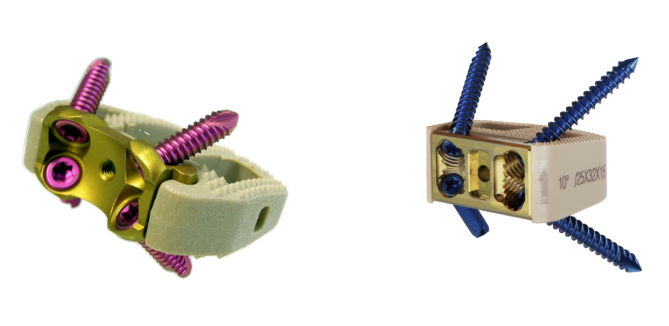
Features: The lumbar self-stabilizing interbody fusion cage is a hollow rectangular fusion device mounted on a titanium alloy plate, with tantalum markers attached. It is used for vertebral body fusion and is available in multiple models with varying heights, surface areas, and lordotic angles to accommodate the anatomical differences among different patients.

Product Registration Certificate